

















The Secret Government Study that Leveraged the Opioid Crisis- THE TRUTH Part II
It was NEVER about ADDICTION. Congress decided to throw the American People under the bus
Calls were ignored.
Politicians sent back form letters.
Specifically, I will never forget Senator Bob Casey sending me a form letter about immigration when I sent him a letter, detailing my hospital stay from hell. Great public servant, Bob. He wears flannel when he visits my hometown. You know, so he can dupe the folks at the Shop ‘n Save into thinking he is like them.
The ACLU National repeatedly refused to help a single incurable painful disease patient. It was “above their pay grade”. Or something.
No lawyer would take a case. Not sexy enough.
Reporters, by and large, jeered at us when we asked for corrections.
Only a very few journalists were brave enough to report real facts, truth, real data.
Daniel Horowitz of Conservative Review was one of those brave few. His series on the so called opioid crisis was superb. He seemed a decent person to those of us who asked questions.
But their few voices were always drowned out by the relentless hammering of The Machine.
There was plainly and obviously something wrong here.
When this concern was voiced, the person voicing it was quickly ridiculed and dubbed a “tin foil hatter”, shown quickly to stage left and told to leave.
Black holed. Even by so-called “pain” groups. What a joke.
I am here to announce we are vindicated.
There indeed is something wrong.
Something damnable.
Something so violating and outrageous, one will scarcely believe it’s true.
But it is.
It’s real. It’s happening. It’s ongoing as I type.
I wish I could say that hitting publish on this piece will end it.
It won’t. Because evil never goes away that easily. Look at the world.
But at least YOU WILL KNOW WHY.
I preface this piece with a truth, somewhat of a disclaimer.
By saying that we real advocates work in the red. No, I am not asking for money. I am telling you that we are real.
Despite what you may have been breathlessly told otherwise. Told by those so called advocates that stay a quarter step behind drama, have a screenshot convenient for every situation, and who work “tirelessly” doing absolutely nothing except keeping good people riled every day on social media.
Do they do anything else but that? No. Simply, no. I suppose they do work tirelessly, just not for you and not for painful disease patient rights.
Self aggrandizement and humble braggadacio via tweet or post is not working for patient rights.
It’s beyond the pale that our own government thinks nothing of using addicts in a “quid pro quo” of their own desperation and paying their own senatorial/representative staffers to pose as “patients with sick wives” to infiltrate painful patient groups and report back all they see and hear.
We don’t get paid for the long hours, nights, and weekends we spend digging up all this… horror. Unsnarling it so we can show you.
It’s… really just that simple.
There will be many damnable, filthy lies, many horrible character assassinations published, texted, whispered regarding me, regarding others, specifically Lauren Deluca and Shasta Rayne Harner, the ones who brought this unbelievable information to me, we all were shocked …who have risked everything, risked it ALL to bring this information to YOU.
Do you think this is not deadly serious? This isn’t a movie, a book, a video game. This is real life, with real people. People they do not give one tiny shred of care about. Because you are watching is the only reason we are breathing. Keep watching.
The government operatives peppering our patient movement who attack advocates, the ones masked as patients… it’s truly unbelievable. The backpedaling, lies, false victimhood, stealing of credit, and backstabbing has begun already in earnest. It is spinning higher and higher.
Please use critical thinking.
That is all I have ever asked of you — as you well know if you have been and are my wonderful follower all this time. I do care about you. I do.
Use your intelligent, common sense, critical thought.
If you are here for drama’s sake?
To hell with you.
Shame on you!
Go back to your pit. I know who you really are. And better yet — who you really aren’t. I have never done a single thing in regards to incurable painful disease patients that would make me ashamed, because I have been fighting for them since I became one and found out my government wanted to kill me. I have never lied or entered a back deal for powerful influence or money. I have never struck a deal to harrass an advocate for money or influence or to be “liked”.
When all this is said and done, I will retreat to my corner of Medium and resume my writing that 20 odd people may read or share. My dream of starting an advocacy group for rare painful diseases has been put on hold because of trolls, likely fake patients.
I am not a CIAAG employee or board member. I am merely a person with which Lauren Deluca and Shasta Rayne Harner share a mutual respect of shared interests and goals, who they approached to help with writing and research.
No one is being paid. Not on our side anyway.
Again- I will gladly share my tax forms this year with anyone who doubts me. It had 0 dollars next to my name for income. Lucky for me, my husband has a good job and supports me financially. I hate not working and I miss it. Advocacy work doesn’t pay bills. Being a turncoat, informant, and online stalker pays bills. Ask them. Have you ever seen them, their faces, in real life? Their taxes, the forms, in real life?
My goal also is to open the door and turn on the lights so the coyotes hiding in the corners and the roaches creeping under the tables come out, desperately trying to flee.
Good advocates have people “assigned” to them, to befriend them or to harass them endlessly.
It’s horrible and also unfortunate to find those you thought were real friends… weren’t. They only “liked” you because they were paid or told to befriend you by evil, corrupt, envious people in attempts to get information.
The real patients will finally know the truth. What was done to them and why. This is for you.
You must check your politics here. There is NO room for partisan politics. Any reference herein to a politician is simply to point out what he/she did, or make fun of them, not to go on a personal belief tangent.
Every one of them suck. They all knew. All of them.
The United States Government, through the CDC, has implemented a massive clinical trial- a population based study, through the creation of the Centers for Disease Control’s 2016 Guidelines for Opioid Prescribing for Treatment of Chronic Non Cancer Pain. The evil plot originated in Washington State. It was hatched to flow through and be included in the ACA, and everything since that awful law was passed marched the country toward this end. The Guidelines were a conduit.
This is real and has been admitted to by our United States Congressional and Senatorial offices.
The PR machine has ran non stop since, spinning desperately to distract you and dismiss what I am telling you, to hopefully deflect blame away from politicians.
They are terrified you will not vote for them next year and likely will throw them out.
What?
What do I mean by this?
The Government (and others) wanted to study pain patients who were using opioids and they wanted to take them off their opioids.
They knew that, well…people like being pain free (and able to work- though they won’t admit that). They wouldn’t sign up willingly for that and they needed a huge pool of people to study.
What better way to get one than to push through horrendous stipulations such as the CDC guidelines… then the National Pain Strategy and…
Watch what happens and record it all. Use it for preventative health, study of disease, and a kind of “pre crime” profiling too.
This is a much faster, easier way… without getting a single signature of consent- that pesky damn informed consent.
That stupid HIPAA. The smoke and mirrors law that no one ever enforces outside a few obvious placaters.
Wanted everyone off opioids to study what happens — and also because they straight up think anyone who uses opioids is an addict, The End. We all are losers who want to get high all day and waste their (insert faux indignation) money.
They knew they could not get volunteers. So instead? They forced a horrific situation upon THE ENTIRE NATION.
That is how much they value each and every person in the vast American public. We who vote for, rally for, and pay for.
Because it doesn’t matter to them. It did not and will not affect their health or their care. They made damn sure of that in the ACA.
As I said in my previous pieces leading up to this one, socialism never affects the self appointed elites. Their personal care and family’s care was never affected. They never writhed in pain.
For crying out loud, the very recent college admissions scandals only underline what I mean when I say they truly believe they are above us all. Nailed here: The True Scandal of the College Admissions Scam — medium.com
Pretty sweet, really kind of our public servants, the ones we pay.
Obama passed the actual laws for them (sorry, guys, but he did) and then they got all their ducks in a row. The previous fellas sure helped, make no mistake.
The ACA (also known as the worst piece of s*** legislation in American History- aka “the insurer handout”) gave broad powers to HHS. To insurers. To private corps, like Appriss.
Well, it’s okay. No one read it. How were they supposed to know, right??? I mean, that excuse they have used for so many things…
Of course, no one said a damn word. They never did about a thing while Obama was President, let’s be real here.
Part and parcel why this plan had to happen during the Obama administration.
This would never squeak by any other White House — even Bill! The media and every person in Congress would be on them like starved wolverines on an injured doe.
HHS never enjoyed such powers as these before. George W. “Mistakes were made” Bush and Darth Cheney had nothing on this… but then again, Cheney shot a man while hunting and walked free.
After he made the man he shot apologize to him. Because, like, manners.
HHS was given powers under the ACA, mostly under Title IV, like:
- Creating the powerful, hidden 15 person “National Prevention, Health Promotion, Public Health Council”.
- Creating the “Center for Medicare and Medicaid Innovation” (with their little subgroup, ‘Institute of Healthcare Improvement’- a bean counter group interested in one thing — cutting costs, lives be damned. How Karl Marx of them!)
- Strategized “Healthy People 2010” a group with faux smiles and one size fits all (socialist) mentality of treatment, grouping all under one treatment model-theirs.
- Creation/Funding the infamous (to the very few advocates who have found this thing and read it) “Living Well with Chronic Illness” e-book/guide through the nefarious “Institute of Medicine” incredibly renamed the “Health and Medicine Division” on March 16, 2016, the same day as the release of the CDC Guidelines. I’m sure that was one of those fantastic coincidences.This publication is not to be confused with the book by author Joanna Charnes that has been mysteriously shoved up HIGH in Google search the past two days. We will come back to this document — note it recommends studying all groups in the USA. Well, except white males. Everyone else though! Hitler 2.0 up in here!
- Developing the “Health in All Policies” approach with CDC, National Prevention Strategy — the government-level way of saying to every single government agency: “Remember in grade school, we all had to use the sh**ty scissors? No one was allowed to bring in a pair? If you were left hand, you got green handles, right hand, blue? Well, this is our scissors policy. Every last one of you is implementing this thing, whether you wanna or not. No crybabies,” announced at a meet of the “National Prevention Council” a snug group of leaders from every single agency in our thoughtful government (sec. 4001 in ACA)- through the Surgeon General’s Agency. His tweets make so much sense through this lens. How dare he!
Since Healthy People 2010, the Institute of Medicine (not whatever that bland, inoffensive name they imagined themselves to be the day the Guidelines they directly caused came out) recommended another initiative — “Healthy People 2020–2030”. Basically an every decade thing.
HHS has given the green light to the Office of Surgeon General that “Health in All Agencies” (HiaA) be used to craft HP ‘30.
And…
Here is where Brandeis and Appriss come in, everyone.
To make sure the goals of these programs created in 2010/2011 were actually being met, of course a surveillance system had to be put into place.
Later on, they could “hook” EHRs into this system, already tailored to carrying electronic information, and call that the gateway. Appriss Gateway, in fact. In 2012 the Kentucky State legislature made a law called the Kentucky State Prescription State Monitoring Compact (not program — COMPACT). There are stakeholders and investors in this compact, with annual reports required and generated. Not a single one of those reports exists for public perusal, nor does even a list of its members exist for review. Requests have been blatantly ignored. Oh, and Appriss is located in Kentucky. Coincidence alert!
The surveillance system was firmly under the care of another congressman, Rep. Hal Rogers– R-KY- Apprissville, Prince of Pork himself. Sure, that is a great idea.
There was the HUGE question of consent, here.
They decided to completely sidestep consent by simply pretending it didn’t exist.
By pretending that a patient who signed a form at that office for their care at that office was somehow informed and understood what was happening and the myriad of ways his/her information would be viewed/bought/sold/studied as part of the PDMP programs.
Hell, the entire premise of what was occurring was already flagrantly so outrageous.
This was nothing. A drip of candle wax on a sh**cake with ten layers.
So, what do we have thus far?
When the ACA was conceived, these people put their plan into play. These innocent sounding orgs were all created under the umbrella of HHS. Powerful men and women came in with an agenda, a very twisted agenda, under the banner of “health and wellness”.
What it really was — eugenics and population engineering, a real time study of genetics and disease markers/ indicators.
To be clear, there is nothing wrong with science. Nothing wrong with study of disease. Nothing wrong with promotion of health and wellness.
It’s all monstrous when it is done to unwitting people. It’s a horror movie when people are used as lab rats and guinea pigs in experiments without their consent or knowledge. It is a crime against humanity to withhold pain medication, “to see” what happens.
Especially when assisted suicide is one of those “whats” on the table — as it is in 8 states now, NJ the latest to topple.
It’s called “gaslighting” in psychology when a person attempts to convince another person a valid, lived experience didn’t actually happen with manipulation and seeds of doubt.
Did the government learn absolutely nothing since Tuskegee?
Since the 70’s with their twisted psych personality shattering garbage goings-on?
Perhaps they did …and this is the result.
I observed before that evil always reinvents itself, improving upon the mistakes of its predecessors.
This is happening today, right now. This is not a “theory” of what happened.
We have the government with stakeholders in insurance and other private entities — but mostly insurance — who met up with physicians and said:
You know? We think these people who take opioids are just a bunch of losers who sit at home getting high all day with our disability and worker’s compensation money, while we pay it every month. We need to get these lazy jerks off their a***s and this is how we are gonna do it. And furthermore, this whole pain meds thing is ridiculous. We don’t need to be paying for pain medication period for all these people. They need to suck it up, buttercup, like their grandmas did, and figure it out themselves. I mean, of course, you know, we will be making sure we have enough for ourselves, but those people need to learn who their betters are somehow, but while we are pushing all this equality s**t.
Here’s how. Make it happen.
Do you even have a clue how much money we will make, oops, I mean, save?
Oregon has it right all along, letting people off themselves. In fact, we sure would LOVE to know how many people would off themselves if they got their pain pills taken away forever. Because that is our national, in fact, World, goal. In both respects. Let’s watch there first. Because we don’t have a solid grasp on these random suicides. CDC isn’t tracking those well enough.
Where is Kolodny in all this? Everyone knows I think Andrew could probably pass the entrance exam for kindergarten. After that, it may get dicey.
I am almost fully certain that Andrew Kolodny will be sacrificed by his handlers in this thing, and in the coming weeks, many incurable painful disease patients will see a vindication the likes of which hasn’t been seen since the news came in they caught Ted Bundy.
Unfortunate, in there is no way on earth this thing could have been machinated by the likes of him, sorry. Anyone with a whit of sense would know that.
However, you reap what you sow, Andrew. Hey, I don’t even think you are smart enough to have even come up with the names of some of these groups, if that is any consolation. I am just an incurable painful disease patient though, so you hold me in the least esteem — and you have spent the last almost 15 years attempting to convince America I am a drug addict who drools when she speaks and is unable to form coherent thoughts. My words are worthless to you.
Who would have ever believed there used to be a time when Roger Chou and Jane Ballentyne thought that painful disease patients could have long term opioids, that it was okay?
They did think this was okay — in 2009. It is simply amazing how all one believes can change like that, because of a “promise” or something else…
The biggest trigger that caused this to be green-lit, no passing go, was the Baby Boomers. Yes, I know. I have those feelings, too, sometimes. I was raised by Boomers.
The Baby Boomers are getting old, though.
The first ones started knocking on Big Government’s door for their money — the money they paid into Social Security and all that jazz in June 2012.
Well, why not? It is not entitlement when you paid your whole life into this system.The Boomers by and large did. They worked.
The Washington greed factory foresaw all their perks, expense accounts, lavish spending going into an endless dark vat that is the Baby Boomers when the realization struck them these few claims were the extreme tip of a monster iceberg with a voracious appetite.
What better way to shut off that faucet? Taking away their pain relief, demonizing opioids, making the senior baby boomers feel like addicts for taking an opioid after years of stability taking one… or not allowing any when the time arrived that one needed it.
Less opioids= pain filled, shorter life expectancy/possible suicide= less benefits paid. More money stays in the life insurance account in DC. Of course, not the Boomers lucky enough to be in Congress, but everyone else.
Health, “Wellness”, Prescribing
The race was then on, the ACA was signed into law. The plan began to hatch all its subplots and subplans.
Stakeholder groups got into the action, and here is where crony capitalism is showcased and shines.
Abt Associates was contracted by the government to help them socially engineer the country into thinking opioids were horrible, filthy things. That anyone who used opioid therapy was a drug seeking addict. That any doctor who wrote a prescription was a “drug dealer in a white coat”. DEA suddenly was off the hook for their monstrous failure in keeping illegal Chinese fentanyl out of our country, as physicians were blamed for the first time in history for the deaths of addicts, even in the face of science.
2013 Asset Forfeiture- Starting in CA, laws were weaponized against physicians, and the DEA used this liberally to seize assets of doctors who they arbitrarily decided to arrest — after they used the (now weaponized) PDMPs (prescription drug monitoring programs). The one-two punch frightened doctors into virtually no prescribing of opioids.
2015-California’s Death Certificate Project is worst of all. A classic case of scare tactics via legislation, the government combs through old death certificates looking for “inappropriate prescribing practices” that “may have contributed to demise”. A sheer fright tactic to keep docs from prescribing — all in the name of this study!! There is no opioid crisis. Just their study! How many physicians are or have been arrested and/ or jailed and/or fined all in the name of this study?!
Brandeis University and Appriss Inc. aligned through Peter Kreiner of Brandeis, worked to implement the mass surveillance of the PDMP system in each state.

Not to mention the myriad of different ways and means of study done through the PDMPs themselves — the aforementioned hyperlink under Dr. Kreiner is to one of those ACA hatchlings that was thrown to the VA, “to assess the impact of the Veterans Access, Choice and Accountability Act of 2014 (VCA) on appropriateness of opioid therapy”.
Not only were the surveillance systems mass implemented without a single signature of informed consent, but the systems themselves were used in countless ways to extract reams of sensitive data from unsuspecting patients and sell it to the highest bidder on the healthcare market, as well as “study” in slanted and biased ways to forward this agenda.
As previously mentioned, Rep. Hal Rogers is the Congressional front man on this. Gubernatorial appointments were made to the KY Prescription Drug Monitoring Compact, a self serving, self enriching stakeholder group slipped through legislation.
We have no way of knowing just what data and where all this information went, because these agencies hide behind so-called “proprietary” algorithms and will not disclose their data fields.
A violation of HIPAA, privacy, human and civil rights that is incalcuble.
Healthy People 2010 was implemented with bright splashy graphics on their website. And we all fall for it every time they pull this crap. I have. We just do.
They do these things and invite public commentary — not because what we say is going to actually shape any policies.
Because we are all part of the study now, and they want us to participate in it.
It is fully Orwell’s world.
They file away the comments and move on to tweak the process based on the feedback- tweak it in a way that we won’t notice what we complained about previously.
It is not us shaping the policy. It is them shaping us through the policy.
HHS does this every time with their TaskForce Public Dockets. They post these for patients, not because they want our thoughtful comments and will listen to what we have to say.
They do this because they are required to do so by the ACA, they have to check off the box and show they received public feedback. No more. Hence why we feel ignored.
Because we are! They have absolutely zero interest in anything we have to say. What we think has nothing to do with what they are doing and will shape none of it.
This ties into the “advocate” clinicians on social media. Many patients believe that the clinicians on social media who are surveying them and studying them are on “their side”.
No.
Use of Social Media as Study Device/ Social Engineering Mechanism
The incurable painful disease patient communities exploded online in the wake of the implementation of the government’s scheme.
This was exactly what the government wanted to happen. They knew that people would be easy to study, manipulate, and also they could use the internet to their advantage socially to a large scale to push through their agenda through social engineering.
HHS and NIH, along with several college and university research departments immediately dispatched a multitude of their “finest”.
To pose as patients, troll agitators, patient sympathizers, advocates, leaders of movements… it is so thick in the incurable painful disease patient advocate movement at this point on social media between several different vested interest groups and the government, that one would be more likely to fall in with a faux advocate or faux patient than one would with a genuinely sick person in need of aid. It’s that disgustingly bad. Add in big pharma and their disinfo agents, and it truly is a hot mess.
Not to mention the junkies and the hypochondriacs that are always attracted to these groups. The junkies were immediately pressed into service. They were put to work as trolls and agitators. Paid in trade or cash to actively go after genuine leaders and effective opioid crisis advocates.
They would troll, agitate, and do as much as they could to get that person banned or deactivated off social media so their voice was silent and doing no damage to the government’s work.
These people would infiltrate every group they could, take screenshots of conversations, cause chaos in their wake wherever they went, and spent all their time on social media pretending to do good while being the very worst of human beings. It’s quite gross, the stunning hypocrisy. Lying about themselves and their lives to ingratiate as closely as they could to as many as they could. Blocking these people was like a death in the family to them. They carried on as though it was.
Many are active at this moment doing this very thing. People love drama. This won’t ever stop. The drama they provide keeps them popular.
The others were far worse.
Researchers swarmed in. Some were pretty open about what they were doing, however, patients mistook that openness to mean that person was working for the patients and helping them “gain their meds back”. Nothing could be further from the truth. These researchers had carte blanche to say whatever they had to. They were to gain the trust of patients so the patients would provide information to them — in the forms of surveys, stories, and infographics. Or better, messages in private groups that would provide a rich tapestry of accentuation to the research papers being written.
This proved to be surprisingly easy. Patients were desperate for someone to validate their experiences, especially an authority figure, someone who was a doctor or professional, and these horrible people played them like a fiddle.
Advocacy statisticians, NIH analysts, physicians from the beginning days in Washington State…so many people in the know would play both ends against the middle, dashing away to write it up and submit their pieces to JAMA, NEJM, and the like, or to provide to other physicians and psychiatrists who needed the information to plug holes in their “research”.
Patients were none the wiser.
ACA 4305 Advancing Research and Treatment for Pain Care Management
The part of the ACA that actually directly addresses pain, pain care and treatment is so short and vague as to render this entire topic rote and meaningless.
The only part of this that would raise any eyebrows to anyone is the little nugget buried in paragraph 2 under subsection (a) under 409J of 4305 says this, “ANNUAL RECOMMENDATIONS. — Not less than annually, the Pain Consortium, in consultation with the Division of Pro- gram Coordination, Planning, and Strategic Initiatives, shall develop and submit to the Director of NIH recommendations on appropriate pain research initiatives that could be under- taken with funds reserved under section 402A(c)(1) for the Common Fund or otherwise available for such initiatives.”
The NIH Common Fund has a person or two masquerading as “advocates” on social media networks. It’s interesting to see the interactions being made with these people, simply because of the shark like social climber personalities known behind the profiles. With the Common Fund funding set up as such and desperation of people for money for their psychosocial projects, one has to wonder where the intersection lies? There is no shame, apparently.
The 6 Building Blocks
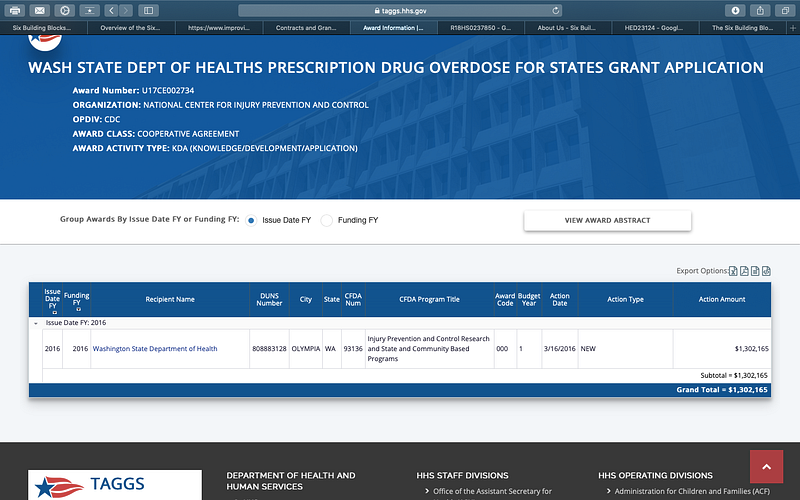
The day of the CDC guidelines were issued, HHS released grant money to the states for the creation of the 6 Building Blocks programs the very next day, March 16, 2016. Of course, this originates in Washington State U and is being sold as a program to help facilitate patient centered care for the complex patient who is on long term opioid therapy. And our friends from Abt Associates are here! Surely this program is in the patient’s best interest.
The Definition of Bravery
The textbook definition of bravery is “the quality or state of having or showing mental or moral strength to face danger, fear, or difficulty.”
I have heard many patients and advocates carelessly say they would do many things… XYZ… if they found out what the “real” story was behind the CDC guidelines.
Well, here is your chance to prove it. I am telling you the story, the truth, and will you do what you have told me all this time?
Jayne Flanders is the co-founder of CIAAG. She is a beautiful, medically fragile young woman with brown hair and a shy smile. Has been with Lauren Deluca since day one, helping her build the little advocacy group from nothing. She has many incurable painful diseases, mostly genetic, and to hear of what she deals with daily makes my heart hurt. Ehlers Danlos Syndrome, Chiari malformation, Hyperadrenergic POTS, are but a few… and yet she works hard at home on this group, often from her bedside, as she is relatively bed bound.
She does all web design, social media content, organization of the web content and analyzing of the data. She works with Lauren Deluca of CIAAG on strategy and all decisions are made together.
Lauren Deluca and Shasta Rayne Harner, two painful disease patients, discovered everything I told you. Two disabled women.
After they discussed it with Jayne Flanders, another disabled woman, they brought it to me, yet another painful disease patient and woman they trusted implicitly.
Then they took it to Washington, D.C. to tell Congress they knew what they were doing.
To tell them to stop.
To tell them enough is enough.
How many more have to die to end the hellish agony their lives had become?! And all for… a study? To save money? Because extremely rich people were greedy and believed a lie?
Imagine two small women walking into Congress and saying what I just told you… right now.
That is what they did.
Because to do what they did… takes courage the likes of which there just isn’t very much of these days.
With courage and determination, they took their research and saw through their task to their goal.
The United States of America owes them a deep and enormous debt of gratitude.
Downloads for all to take to their physician, to hand out, et al… are available for free on CIAAG www.ciaag.net
Now is the time to show solidarity as we unite. Our physicians need this. Our pharmacists need this. How dare they perpetuate this on a free society! Please spread this far and wide!
Use the hashtag #ViolationofANation to get their attention and let them know you know! Get it trending!
I will keep you all up to date on this profile as developments are forthcoming.
Heather Wargo is a Medium Top Writer in Government, Politics, Health, and Social Media. She is a freelance writer and advocate for incurable painful disease patients and physicians affected by governmental overreach.
Heather Wargo has been published by The Western Journal, Lifesite News, The Ascent, P.S. I love You, Publishous, Uncalendared, The Writer’s Cooperative and Writer’s Guild.
Filed under: General Problems | 4 Comments »









