










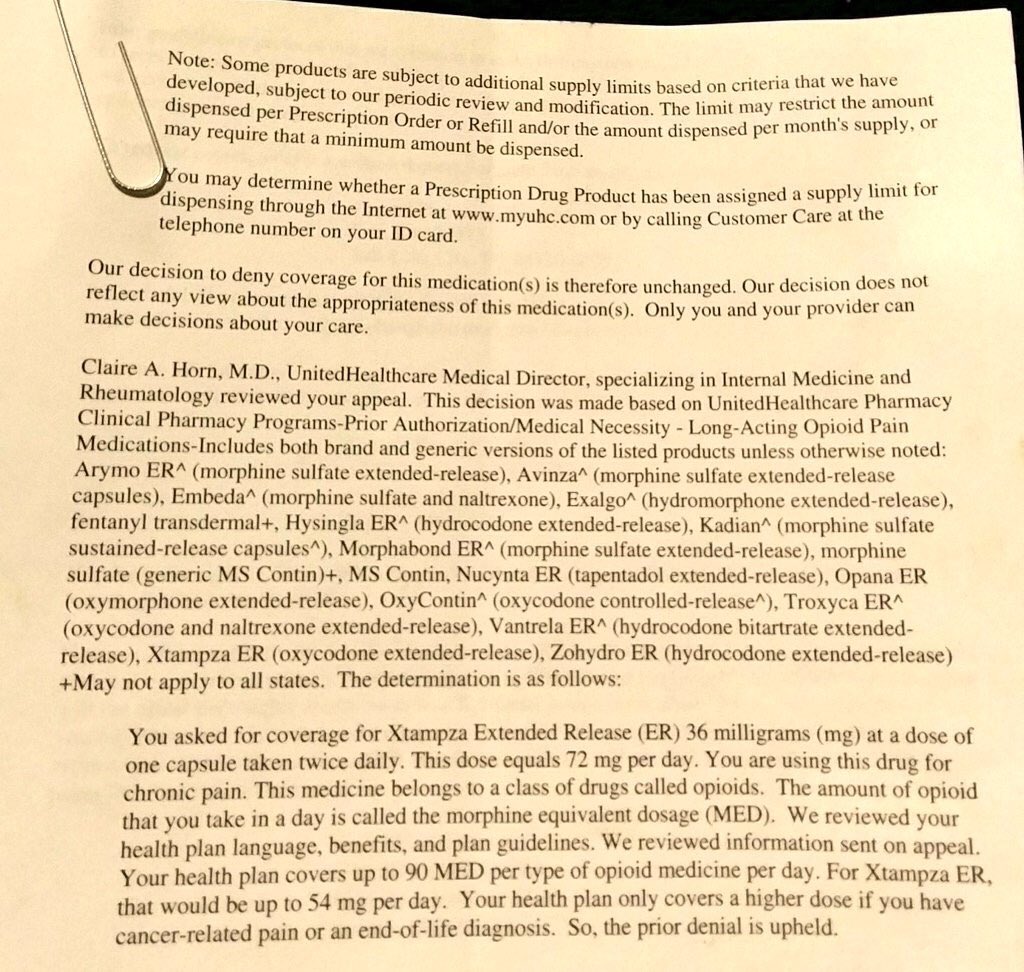

One of the basics of the practice of medicine is the starting, changing, stopping a pt’s therapy. Within the Controlled Substance Act.. it is specific that no prescriber may prescribe for a pt that they have not done a IN PERSON PHYSICAL EXAM… according to this letter is would appear that Dr. Clarie Horn, MD is approving – or disapproving – controlled medications for pts in which she has only “REVIEWED” this pt’s medical records.
According to this https://www.vitals.com/doctors/Dr_Claire_Horn.html#!
Dr Horn has offices in Indianapolis, IN and Dallas, TX… so apparently she is currently licensed in those two states. So unless she is making medical decisions on pts located in IN or TX… – unless she is licensed in other states – then she would be attempting to practice medicine in states in which she is not licensed. Which is ILLEGAL …
 These decisions by some physician employed by some insurance and/or PBM’s who are trying to practice medicine in areas and in means that they are not licensed to do. Perhaps pts who are beneficiaries of these insurance companies who they are attempting to practice medicine on… perhaps they should start filing complaints with medical license boards of the states these doctors are licensed in and the state in which the pt resides.
These decisions by some physician employed by some insurance and/or PBM’s who are trying to practice medicine in areas and in means that they are not licensed to do. Perhaps pts who are beneficiaries of these insurance companies who they are attempting to practice medicine on… perhaps they should start filing complaints with medical license boards of the states these doctors are licensed in and the state in which the pt resides.
More of these corporations get by with what they are doing because no one challenges them… so like most corporations… they will push the envelope as much as they can… “laws are for the little people ” … until they are challenged and some agency tells then to cut the crap out.
Filed under: General Problems







I no longer contribute money to AARP over their false claims regarding opioids in their publication. It seemed to me as if they were trying to scare opioid naive older patients. Also, chronic pain patients need to boycott CVS!
Dr. Horn is not considered to be Practicing Medicine when she is working at her job for UnitedHealthCare.
Then what is she doing ?
You would have to read her job description with United to know what she was hired to do.
She is not diagnosing, treating or correcting human conditions, ailments, diseases, injuries, or infirmities. Therefore she is not Practicing Medicine Denying a claim Is not diagnosing, treating or correcting. Some may view it as that. But, they are wrong.
You are correct, I have re-read the letter and it would appear that some “committee” made up of some unknown/faceless/nameless persons employed by UHC… and they have made the medical/policy decision that non-cancer chronic pain is a non-treatable health issue – in regards to the use of opiates long term. They have also seem to have made the determination that the intensity of non-cancerous pain can NEVER approach that of cancerous pain. Since chronic pain pts are a protected class under the Americans with Disability Act and Civil Rights Act.. if UHC is not imposing the same/similar limitations on the treatment of other chronic health issues.. then it would appear that this is something that is going to have to be adjudicated in our court system. In this letter UHC is CYA when they state that “Only you and your providers can make decisions about your care”… and the DEA considers it a RED FLAG when a pt pays cash for a controlled substance when they have insurance and I suspect that the fact that the pt’s insurance declined coverage will influence their decision on this matter.. and RED FLAG could have a negative impact on the pt, the pharmacy and the prescriber.. UHC… will have near ZERO chance of involved with a RED FLAG. As a reminder to anyone reading this… UHC is the largest Part D provider and is endorsed by AARP… how many MILLIONS in the 50+ age bracket that AARP claims to look out for their best interest… are chronic pain pts ? Does AARP endorsing UHC meet that mission statement ?
Those with disabilities,are protected. in certain situations. But, an insurance company denying certain opiate prescriptions for chronic pain patients is not a violation of the ADA.
Patients that are denied coverage of their opiates. Need to get and keep a copy of the paperwork stating they were denied. That explains why they paid cash. They need to give their doctors a copy. Although chances are the insurance company will notify the doctor of the denial and the reason(s).
There may be a code pharmacists use when they put prescriptions in their states PMP..That code would mean it was denied by the insurance company. And would explain why the patient paid for it.
AARP had an article last year about opioids. Remembering the article, I am 99% sure AARP would have no problem with UnitedHealth care’s new policy. But, even if they did. AARP cannot dictate decisions UnitedHealthcare makes
when a insurance company discriminates against a whole class of pts… that is when ADA/CRA will kick in… since most controlled substances are prescribed to those who are dealing with subjective diseases. From the letter that was posted.. .there is apparently no consideration of daily dose limits with pts who are fast/ultra fast opiate metabolizer. They are using conversion tables that have “fine print” that states they are “fuzzy math” at best.. The print outs by the PMP’s that I have seen… at best – they say that it is billed to a third party or cash.. I am not aware of any override to the PMP by the pharmacist. The DEA considers data-mining as proof of “probable cause”… and pts show up with a TP paying for their non-controlled meds and the pt paying cash for controls… My money is on that they will not look for – or care about – mitigating circumstances. Then they will be going after pharmacies and docs for failing to meet the “corresponding responsibility” requirement in the CSA. In reading the letter… it is clear that it had the “blessing” of one or more attorneys trying to CYA UHC… but … IMO.. too many pts will have their quality of life and/or their family’s financial well being compromised by UHC decisions… but.. there are too many entities going down this same path and so many deep pockets for plaintiff’s attorneys to go after… would not be surprised to see some class action lawsuits. There is a growing list of “bad actors” and the number of pts being adversely effect… is growing exponentially .. a critical mass that starts getting the attention of attorneys… is not that far in the future.
If an insurance company has reason to believe dosage puts the patient at risk, They can deny the prescription.It is not discrimination for a insurance company to deny patients prescribed high doses of opiates. Insurance companies imposing limits on opiates has been going on for many years. They have just added to what they have reason to believe puts patients at risk.
Patients quality of life and families financial well being is not the responsibility of an insurance company, pharmacists or providers.
The DEA is not going to go after doctors and pharmacist due to one red flag from patients paying cash when their insurance companies deny coverage.
https://deachronicles.quarles.com/2013/08/a-pharmacists-obligation-corresponding-responsibility-and-red-flags-of-diversion/
https://secure.in.gov/pla/files/DEA_Practitioner_Manual.pdf
Since those two links are 5 and 12 yrs old respectively… they may or may not have any relevance of the DEA today… AG Session has indicated that he wants to ramp up Civil Asset Forfeiture to FULL TILT and he has also indicated that he believes that the opiate crisis has and continues to be caused/fuel by legally prescribed opiates.. No one knows where the DEA is going… The DEA is not going after a single pt … but.. in data mining the DEA will isolate docs or pharmacies that are prescribing/filling opiates for pts that are paying cash… since UHC is the LARGEST Part D provider… and the top three (CVS Health, Humana ) account for the majority of Part D claims… and they all implement similar opiate dosing policies.. it won’t be hard for the DEA to have their first data point to start their data mining. Of course, the DEA could determine that prescribing/filling above the insurance’s daily limits could be “excessive amounts” and seek to shut down these “pill mills”… To act the DEA doesn’t seem to need facts.. just opinions…
Interesting your statement that insurance, pharmacy or providers have no responsibility for the pt’s quality of life because CMS is starting to impose financial penalties on those three entities if pts are non compliant with their anti-hypertensive meds, diabetic meds, and lipid lowering meds… and they have started a STAR RATING system that if pts complain too much about how they are being treated.. they will loose stars… and loose reimbursement..
Both links are current.
Insurance companies not paying for a specific treatment that they have reasons to believe are dangerous to the patient. Is not discrimination.
Patients non compliance with anti-hypertensive, diabetic and lipid lowering drugs can be costly to Medicare. Patients not receiving high doses of opiates does not cost Medicare anywhere near as much. But patients taking too may opiates is very costly to Medicare. So is the cost of drug rehab.
Under the circumstances. I do not see providers losing stars because patients complain they can’t get the opioids they want for their chronic pain.
You have to look at situations from more than one view point. You also have to be objective. Government agencies and those that must follow their rules are not emotionally involved. And nothing is going to change that.
Wonder why then, UHC would bother to employ an “MD” for such a job position?
It is not unusual for companies to hire doctors for their education, training and experience. But, that does not mean they are Practicing Medicine.
here is a list of physical/mental complication of UNTREATED PAIN… shouldn’t cost much from $$$ standpoint to treat in the longer term.. that is .. unless the pt commits suicide…